- Visibility 198 Views
- Downloads 39 Downloads
- DOI 10.18231/j.jpmhh.2024.017
-
CrossMark

IT-based health event surveillance in mass gathering - Kumbh Mela 2021, Haridwar, Uttarakhand
- Author Details:
-
 Pankaj Kumar Singh *
Pankaj Kumar Singh *
-
Akhilesh Tripathi
-
Rajeev Sharma
-
Meera Dhuria
Introduction
The World Health Organisation defines mass gatherings (MGs) as a “concentration of people at a specific location for a specific purpose over a set period of time which has the potential to strain the planning and response resources of the country or community”.[1] Mass gatherings (MGs) for religious events are a source of religious and cultural tourism within the country of origin and abroad. They involve an influx of a large number of people to a fixed site for a specific duration. The increase in crowd density can have health implications for communicable disease transmission due to the increase in intermixing of healthy and diseased populations and exposure to microbes; this also places a strain on the existing medical care and water and sanitation services, as well as entailing an increased threat of mass casualties due to stampede[1] They pose risks to health security that can cause the health of the populations to be in danger, thereby leading to economic disruptions on a regional as well as global scale.[2]
Mass gatherings can present important public health challenges related to the health of attendees and of the host country population and health services.[3] Public health risks associated with mass gatherings are well documented and encompass a variety of focus areas, from environmental health hazards to infectious diseases.[4] There are many factors determining the risk of a potential infectious disease event in the context of a mass gathering. These include endemic diseases, the number and origin of expected visitors, risk behaviour, language barriers and the demographics of the population involved, as well as the type of event, geographical location, season and preparedness of the public health system in the host country.
MGs present surveillance challenges quite different from routine outbreak monitoring, including prompt detection of outbreaks of an unusual disease.[5] An influx of a large number of people at MG events poses a significant public health risk to visitors and the local population, and places strains on the health systems. It can also threaten global health security due to the potential for rapid spread of high-consequence pathogens following inadequate preparedness. Public health surveillance and response capacity are critical at such MG events for managing public health threats.[6] With the advent of Novel Corona Virus 2019 (COVID-19) the risks posed by Mass Gatherings was increased double-fold. Not only there was a risk of increasing the severity of the pandemic but also there can be an added incidence of other diseases.
The Kumbh Mela is a large religious mass gathering event organised in India.[7] The Kumbh Mela is a religious event in India that constitutes the largest number of people gathered at a specific place and at a specific time.[8] The Kumbh Mela is an ancient Hindu religious riverside pilgrimage held for 3 months, usually at a fixed astrological time. The Kumbh Mela venue rotates between Haridwar in Uttarakhand on the bank of the Ganga River, Prayagraj in Uttar Pradesh on the banks of the Ganga, Yamuna, and Saraswati, Nasik in Maharashtra positioned on the banks of the Godavari River and Ujjain in Madhya Pradesh on the bank of the Shipra River. Bathing in these rivers during the Kumbh Mela is considered an endeavour to cleanse both body and spirit (Rana Singh, 2013; Dubey, 2001). [9] Such MGs imposes substantial difficulties for the accommodation and flow of people. [10]
The Kumbh Mela had to be planned and organised under unusual circumstances because of COVID-19 pandemic. The ongoing spread of COVID-19 infection at such a large gathering would present an additional risk and threat to public health. The two most significant factors at large gatherings that contribute to the increased transmission of communicable diseases are high crowd density and increased population mobility. Usually, the Kumbh Mela is organized for 3-4 months but in the amid of COVID-19 pandemic, the State Government of Uttarakhand decided to restrict it for one month only i.e. From April 01 to April 30, 2021 in Haridwar, Uttarakhand, India.
Huge mass gatherings such as Kumbh Mela requires addressing a broad range of public health risks ranging from outbreak of communicable diseases to loss of lives due to manmade and natural disasters. Public health preparedness is required on a range of potential threats. With MG events such as the Kumbh Mela potentially involving millions of people arriving from anywhere in the country or from around the world, public health surveillance systems were needed that can provide rapid health surveillance information.[11] Public health surveillance should be implemented at mass gatherings to facilitate early detection of outbreaks and other health-related events and to enable public health officials to respond in a timely manner. [12]
Mass gatherings can provide an opportunity to strengthen public health systems. However, they can also introduce new and challenging risks that need to be managed. Due to the possibility of spreading epidemics, the primary focus should be on identifying the potential risk factors and implementing appropriate preventive measures. [13] To address these challenges, a special IT based public health surveillance system was established during Kumbh Mela-2021, Haridwar for surveillance of epidemic prone diseases with major focus on Covid-19 and early response and control of communicable disease threats.
Materials and Methods
A special IT based public health surveillance system was established for the Mass Gathering site at Kumbh Mela, Haridwar using Integrated Health Information Platform (IHIP) under Integrated Disease Surveillance Programme (IDSP). The Integrated Health Information Platform (IHIP) is a web-enabled near-real-time electronic information system that is embedded with all applicable Government of India's e-Governance standards, Information Technology (IT), data & meta data standards to provide state-of-the-art single operating picture with geospatial information for managing disease outbreaks and related resources.
The special surveillance module of IHIIP was created for the Kumbh Mela, comprising 24 diseases specific to Mass Gatherings. For robust disease surveillance, the standard case definitions were formulated by State IDSP Unit and made available at IHIP for easy accessibility. Kumbh mela area was divided into 4 zones with total 75 health facilities (public & private) reported to the IHIP. Once the framework for the surveillance system was developed, the capacity building of Rapid Response Teams (RRTs) and health professionals on standard case definitions, outbreak investigations, laboratory diagnosis and data entry on IHIP was conducted.
A field public health emergency operations centre (PHEOC) was established at Kumbh Mela site, and a team of public health experts were posted to monitor the COVID-19 and other disease situations. The PHEOC was divided into two main components: IT-enabled data surveillance and Watch Desk. The PHEOC was set up and connected so that the Watch Desk received information from the devotees, field healthcare units, IHIP portal, the media, and the control room run by the state administration. Mechanisms were also set to ensure communication between the Data Surveillance unit and the Watch Desk for effective and timely response to public health emergencies.
Results
The special IT based surveillance monitored 24 diseases/syndromes using standardized case definitions. The Kumbh mela area was divided into 4 zones. A total of 75 health facilities identified in all 4 zones ([Table 1]). Real time data reporting was done from all identified health facilities. Analysis of reported surveillance data was conducted and feedback of the same was disseminated by the PHEOC. [Figure 1] shows the data flow and feedback mechanism from RUs to the PHEOC.
|
Zone |
Number of Health Facilities |
|
Zone-1 |
42 |
|
Zone-2 |
6 |
|
Zone-3 |
17 |
|
Zone-4 |
10 |
|
Total |
75 |
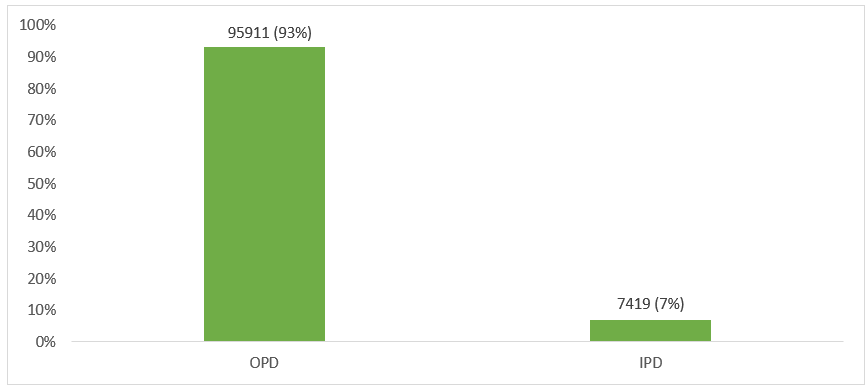
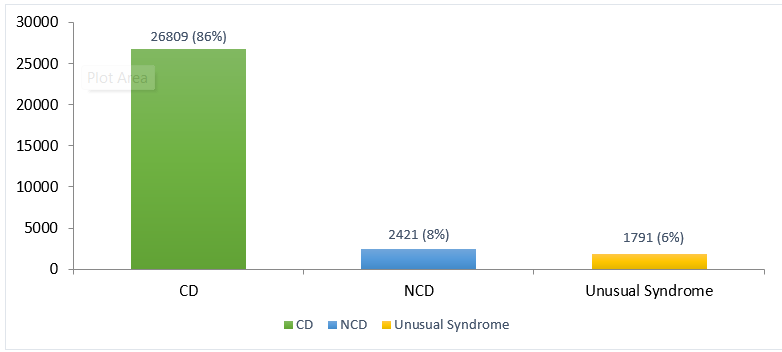
From April 01 to April 30, 2021, a total of 103330 hospital encounters were reported on IHIP, of which 95911 (93%) from OPD and 7419 (7%) from IPD ([Figure 1]). Out of total 103330 hospital encounters, 31021 cases of the listed diseases/syndromes were reported on IHIP of which 26809 (86%) communicable diseases (CDs), 2421 (8%) non-communicable diseases (NCDs) and 1791 (6%) unusual syndrome ([Figure 2]).
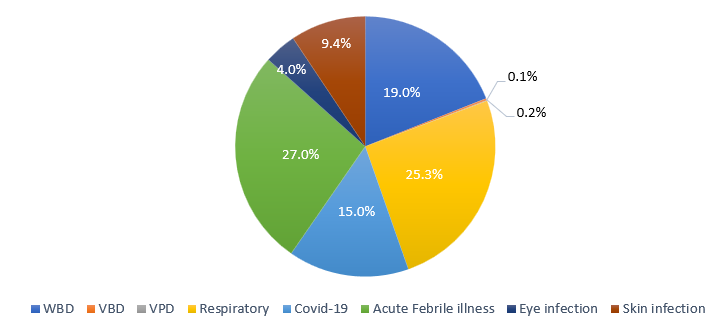
Among the total reported cases of communicable disease (n=26809), acute febrile illness (n=7233, 27%), acute respiratory illness (n=6793, 25.3%), water borne diseases (n=5086, 19%), COVID-19 (n=4025, 15%), skin infections (n=2512, 9.4%), vector borne diseases (n=66, 0.2%) and vaccine preventable diseases (n=19, 0.1%) encountered ([Figure 3]).
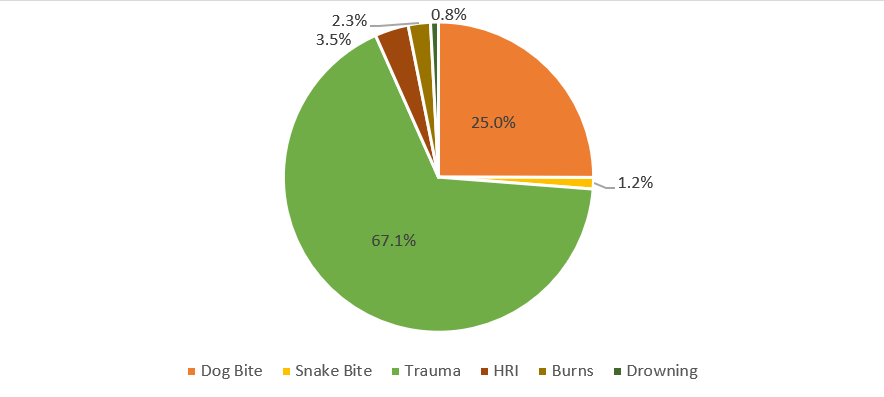
Out of total non-communicable diseases (n=2421), trauma (n=1625, 67.1%), dog bite (n=606, 25%), heat related illnesses (n=85, 3.5%), burns (n=56, 2.3%), snake bite (n=29, 1.2%) and drowning (n=20, 0.8%) were reported ([Figure 4]).
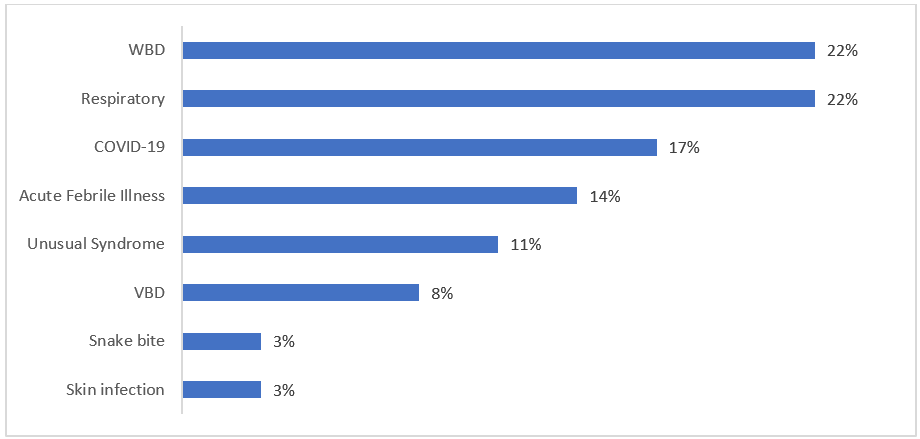
A total of 36 early warning signals (EWS) generated and responded, of which 8 (22%) of WBDs, 8 (22%) of ARI, 6 (17%) of COVID-19, 5 of (14%) AFI, 4 (11%) of unusual syndrome, 3 (8%) of VBDs, 1 (3%) of skin infections and 1 (3%) of snake bite ([Figure 5]). Due to early detection and timely response, there were no outbreak reported.
Conclusions
In the past, the administrations of the host states have organised and managed the Mela efficiently. However, in 2021 due to COVID-19, the Kumbh Mela had to be organised and managed in novel circumstances. With a gathering so large, the continued transmission of COVID-19 infection would pose an additional public health threat. High crowd density and increased population mobility are the two most important factors at mass gatherings that contribute to the enhanced transmission of communicable diseases. In such situation, a robust mechanism for disease surveillance, capacity building of the public health workforce, collaboration of stakeholders and infection prevention was developed and implemented during Kumbh Mela 2021, Haridwar.
The IT based real time disease surveillance system i.e. IHIP was successfully implemented in Kumbh Mela-2021 for early detection, monitoring and quick response to public health threats. The special disease surveillance helped in monitoring health event alerts and health condition alerts. The real time reporting on IHIP resulted in quick data analysis and public health response.
The PHEOC monitored early warning signals and facilitated early detection and quick response to public health threats. The Rapid Response Teams responded, and essential public health interventions were taken in a timely manner to the reported early warning signals, so that not a single event is converted into an outbreak. Surveillance data were useful for public health action with early detection and response. Daily disease situational analysis report was generated to highlight the real-time health risk during the Kumbh.
Acute febrile illnesses emerged as a leading cause of morbidity. Future Mass Gathering events like Kumbh Mela should include real time-based disease surveillance system as part of planning and augment capacity to diagnose and management of acute febrile illness.
Source of Funding
None.
Conflict of Interest
None.
Acknowledgement
We would like to acknowledge support of World Health Organisation, Ministry of Health and Family Welfare, Government of India, Other departments of Government of Uttarakhand and all others who are directly or indirectly engaged in successful implementation of the above special mass gathering surveillance system.
References
- World Health Organisation. Key planning recommendations for mass gatherings in the context of COVID-19: Interim guidance. 2021. [Google Scholar]
- World Health Organisation. Global mass gatherings: implications and opportunities for global health security. 2011. [Google Scholar]
- World Health Organisation. Public health at mass gatherings: key considerations. World Health Organization. 2015. [Google Scholar]
- V Diwan, U Sharma, P Ganeshkumar, JW Vivian Thangaraj, S Muthappan, V Venkatasamy. Syndromic surveillance system during mass gathering of Panchkroshi Yatra festival, Ujjain, Madhya Pradesh, India. New Microbes New Infect 2017. [Google Scholar]
- SR Mekaru, K Khan. Anticipatory surveillance for mass gatherings: a novel application of mass media surveillance. Emer Health Threats J 2011. [Google Scholar]
- V Aggrawal, T Dikid, SK Jain, A Pandey, P Khasnobis, S Choudhary. Disease surveillance during a large religious mass gathering in India: The Prayagraj Kumbh 2019 experience. Int J Infect Dis 2020. [Google Scholar]
- A Baranwal, A Anand, R Singh. Managing the Earth’s biggest mass gathering event and WASH conditions: Maha Kumbh Mela (India). PLoS Curr 2015. [Google Scholar] [Crossref]
- S David, N Roy. Public health perspectives from the biggest human mass gathering on earth: Kumbh Mela, India. Int J Infect Dis 2016. [Google Scholar]
- RPB Singh. . Hindu Tradition of Pilgrimage: Sacred Space and System 2013. [Google Scholar]
- K Jani, D Dhotre, J Bandal. World’s largest mass bathing event influences the bacterial communities of Godavari, a holy river of India. Environ Microbiol 2018. [Google Scholar]
- MP Cariappa, BP Singh, A Mahen, AS Bansal. Kumbh Mela 2013: healthcare for the millions. Med J Armed Forces India 2015. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Surveillance for Early Detection of Disease Outbreaks at an Outdoor Mass Gathering- Virginia. MMWR Morb Mortal Wkly Rep 2005. [Google Scholar]
- S Sridhar, P Gautret, P Brouqui. A comprehensive review of the Kumbh Mela: Identifying risks for spread of infectious diseases. Clin Microbiol Infect 2015. [Google Scholar]