- Visibility 392 Views
- Downloads 60 Downloads
- Permissions
- DOI 10.18231/j.jpmhh.2024.018
-
CrossMark

Hyperbilirubinemia and transaminitis in hepatitis A: case report on early remission through ayurveda interventions
Abstract
Background: Hepatitis A is a common cause for acute hepatitis and jaundice. It is mostly self-limiting requires no or suppurative treatment and very rare cases prolong jaundice, liver failure and death. Prolonged jaundice types of cases are mostly going to folk healers and herbalist. Ayurveda has no recordable evidence of course of treatment in Hepatitis A. Therefore, this case paper will be a notable evidence for Ayurveda in hepatitis A.
Case Presentation: A 43-year female came to hospital with an one week history of lethargy, anorexia, weight loss and yellow discoloration of urine. The patient has Hepatitis A (HAV) IgM antibody positive with other viral profile negative and elevated bilirubin(6.28mg/dl) and high transaminase (SGOT-824U/L and SGPT 1263 U/L).
Medication and Uutcome: Arogyavardhini Vati, Liv 52Hb and Phalatrikadi Kwatha were administrated in its standard doses as these regimen have Agnideepak(Carminative), Srotosothaka (channel purifier), Mrudu virechana ( Mild purgative)properties, but no signicant change in liver function test . then ( Siddha Makardwaja Rasa) is added to reduce liver inflammation and possible involvement of cholangitis. The physical strength , appetite was normalised along with normalisation of bilirubin and liver transaminase within three weeks of the therapy.
Discussion: The combination of therapy may reduce the bile acid cytotoxicity of bile and, possibly, decrease of the concentration of hydrophobic bile acids in the cholangiocyte. As Siddha Makardwaja special is in metallic oxide form (Au/HgO), it may be acts as an anti-inflammatory drug by reducing pro inflammatory cytokine expression, blocking leucocyte adhesion and decreasing oxidative stress due to infection.
Conclusion: This case report is preliminary evidence for further stresses the significance of Siddha Makardwaja Rasayana along with other Ayurveda formulations in early remission of high bilirubin and liver transaminase in Hepatitis A infection. This treatment regimen can be used for local epidemic of Hepatitis A for appropriate Ayurveda management after randomised clinical trial.
Introduction
Hepatitis A is a common cause for acute hepatitis and jaundice. It is known for its epidemic jaundice and transmission by the faecal-oral route (either via person-to-person contact or consumption of contaminated food or water). Its prevalence is high in developing countries. It starts from loss of appetite, nausea, fever, malaise, abdominal upset along with dark urine, pale stool and jaundice. It is mostly self-limiting requires suppurative treatment and very rare cases liver failure and death.[1] Adults have signs and symptoms of illness more often than children. The severity of disease and fatal outcomes are higher in older age groups. Generally, bilirubin and transaminase decline after two weeks, normal biochemical shown in two to three months and complete recovery in six months. In some rare cases prolonged hyperbilirubinemia (≥5mg/dl) and elevated transaminase (Transaminitis) in a complication of hepatitis A (HAV) regarded as cholestasis hepatitis.[2] The diagnosis is detection HAV -specific immunoglobin G (IgM) antibodies in blood, reverse transcriptase polymerase chain reaction (RT-PCR) to detect the hepatitis A virus RNA and ultrasound of liver for exclusion of obstruction pathology. The modern medical literature described oral steroid for treating cholestasis hepatitis.[3] One survey study revealed that more than 73% patients effected from hepatitis A epidemic were relieved from Ayurveda Treatment.[4] Hepatitis viral infection can be grouped under Krimija Yakrit roga.[5] Infective hepatitis has good clinical response in Ayurveda and Korean traditional medicine successes has excellent result to rescued from epidemic.[6], [7], [8] The search of potential herbal compound as anti-hepatitis A from Ayurveda products or natural product are less focussed possibly the mitigation of infection through vaccine.[9], [10] There is no specific treatment for hepatitis A. Recovery from symptoms following infection may be slow and can take several weeks or months. Many patients come for Ayurveda treatment for early remission of Jaundice.[11] Hepatitis A causes various gastrointestinal and systemic symptoms, so herbal medicines composed of multi-compounds can be useful in hepatitis.[12], [13] There is no solitary evidence of Ayurveda medications in Hepatitis A infection is found in current literature survey. Therefore, this case report is planned to evaluate the Ayurveda treatment outcome in hepatitis A infection. In this article, a case report of Hyperbilirubinemia and transaminitis in hepatitis A infection presented, which has good early response through Ayurveda treatment.
|
Time in Days |
Clinical findings |
Intervention |
|
(10/2/2024) |
Yellow dislocation sclera, urine, anorexia, nausea itching, |
No intervention Advise for LFT & Hepatis virus panel serology |
|
D0 (12/2/2024) |
Deranged LFT & Positive Hepatitis A (HAV) IgM antibody |
Arogyavardhini Vati 250mg tab twice daily |
|
|
|
Liv 52 Hb – 1 tab twice daily |
|
|
|
Phalatrikadi Pachana 30ml twice before food For one week |
|
D8 (20/2/2024) to 02/3/2024 |
Patient felt more weakness, dark urine and clay-colored stool. Adv sonography of Abdomen |
Added 1. Siddha Makardwaja Rasa 125mg tab twice before food for ten days Liver sonography-normal |
|
D19(3/3/2024) |
Felt better,Normal liver enzymes |
Stop all medications Observe for two week |
|
14/3/2024 |
Normal diet and life style |
No medication |
Patient Information
A 43 year female came to hospital with an one week history of lethargy, anorexia, weight loss and yellow discoloration of urine. The patient has no significant past medical history taking any herbal or synthetic drug and her family members are healthy.
Clinical Findings
The patient was pallor, icteric and slight febrile. Her abdomen was tender at epigastric region. No hepatosplenomegaly or lymphadenopathy was noted. The patient was sent for Hepatitis virus panel, liver function test and complete blood count for further evaluation. The laboratory finding showed deranged hemogram and LFT ([Table 2]). The Hepatitis A virus (HAV) IgM antibody positive with HbSAg and HCV are negative.
Time Line
The patient’s liver function test was elevated after initial treatment and rapidly corrected after the administration of Siddha Makardwaja Rasa ([Table 1])
Diagnostic Assessment
Hepatitis A diagnosis was made by clinical symptom of jaundice along with Positive Hepatitis A (HAV) IgM antibody and elevated bilirubin and liver transaminase. The assessment was done based on clinical symptoms and liver function test. The patient was advised to take follow up visit in every week and if any deuteriation of health status then visit immediately.
Therapeutic Intervention
In this present case, planned for Agnideepak(Carminative), Srotosothaka (channel purifier), Mrudu virechana ( Mild purgative) then balya (Immuno booster). Arogyavardhini Vati has been used in viral hepatitis and it has Agnideepak(Carminative), Srotosothaka (channel purifier), Mrudu virechana ( Mild purgative)properties. [14] Liv 52Hb can reserve oxidative damage of hepatocytes and hepato protective action, it has good clinical outcome in hepatitis B infection. [15] The concept of Sopha and inflammatory mechanism have a crucial role in hepatitis A, [16] Therefore a good systemic anti-inflammatory medication in form of nano particle ( Siddha Makardwaja Rasa) is added to reduce liver inflammation. [17] Phalatrikadi Kwatha is a pitta hara and rechana drug [18] and its ingredient tripha is already used in Hepatitis A in Kerala.
Follow up and Outcome
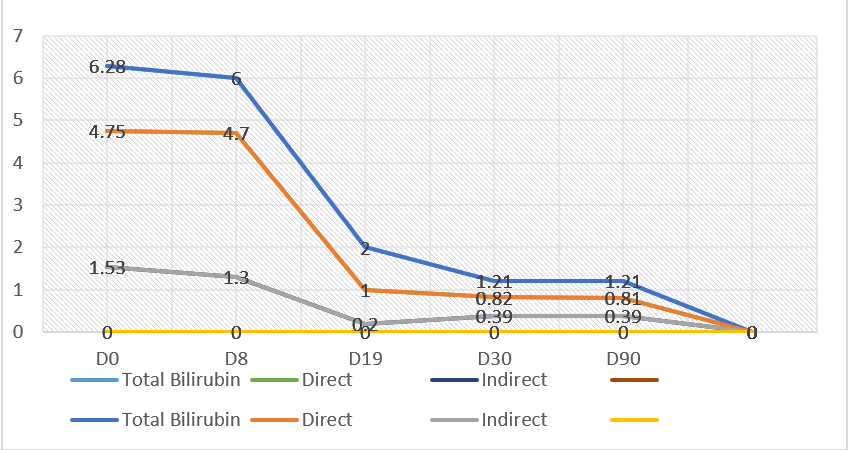
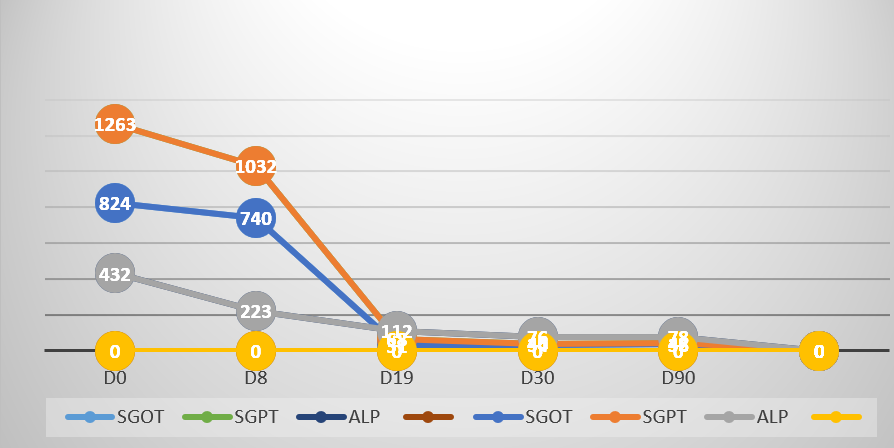
Based on the presenting system and clinical examination the patient was diagnosed as Kamala caused by Hepatitis A infection. The patient base line clinical profile and symptoms had hyperbilirubinemia (6.28 mg/dl) and high transaminase (SGOT-824U/L and SGPT 1263 U/L), but no significant change after 8 days administration of Ayurveda medications may be the natural course of disease process ([Table 2]). Therefore, a systemic anti-inflammatory and immune modulator i.e Siddha Makardwaj special (in tablet form of Zandu Pharmacaeutical) 125mg tab was administrated for ten days. There is a significant and rapid reduction of bilirubin and liver transaminase in ten days and the appetite, strength normalised ([Figure 1], [Figure 2]) The medications were stopped with an advice to consult after ten days. The patient was followed for three months and no relapse of jaundice was noted. The sero conversion was after 90 days of natural course of disease.
|
Laboratory Parameter |
D0 |
D8 |
D19 |
D30 |
D90 |
|
Hb% (g/dl) |
9.2 |
8.8 |
9.0 |
10.2 |
10.6 |
|
Total Leucocyte count |
8400 |
8200 |
7800 |
6600 |
6600 |
|
Total platelet count |
223000 |
220000 |
260000 |
260000 |
270000 |
|
Total Bilirubin (mg/dl) |
6.28 |
6.0 |
2.0 |
1.21 |
1.21 |
|
Direct (mg/dl) |
4.75 |
4.70 |
1.0 |
0.82 |
0.81 |
|
Indirect (mg/dl) |
1.53 |
1.30 |
0.2 |
0.39 |
0.39 |
|
SGOT (U/L) |
824 |
740 |
31 |
34 |
36 |
|
SGPT(U/L) |
1263 |
1032 |
68 |
40 |
42 |
|
Alkaline Phosphatase (U/L) |
432 |
223 |
112 |
76 |
78 |
|
FBS (mg/dl) |
88 |
78 |
82 |
84 |
82 |
|
S .Urea (mg/dl) |
24 |
23 |
25 |
26 |
23 |
|
Creatinine (mg/dl) |
0.78 |
0.8 |
0.6 |
0.8 |
0.8 |
|
PT |
13.8 |
13.2 |
11.2 |
11.00 |
11.00 |
|
HAV (Ig M antibody) |
Positive |
- |
- |
Positive |
Negative |
|
USG of Abdomen |
|
Hepatomegaly |
|
|
|
Discussion
In this paper, it was reported on the presentation of an elderly patient with an acute HAV infection. A presumptive diagnosis of hepatitis A was made based on the patient’s historical of symptomatology, coupled with supporting laboratory findings. Hepatitis A infection range from asymptomatic infection to Acute Liver Failure (ALF), but it does not progress to chronic hepatitis. However,10%–20% of patients develop relapsing hepatitis or pro longed cholestasis lasting for more than 6 months. Hepatitis A-associated ALF may rapidly progress within a week. In hepatitis A patients, serum levels of several cytokines and chemokines are increased compared with healthy controls.[19] Ayurveda medications for Kamala (Jaundice) widely practiced by traditional healers rather than qualified Ayurveda practitioners. The proper hepatitis A diagnosis with clinical progression and treatment outcome in Ayurveda is not found in modern literature. The initial treatment regimen is not responded well may be due to natural progression of disease to cholestasis with hepatomegaly. The induction of Siddha Makardwaj special contains gold nano particle in metallic oxide form (Au/HgO) which have proven anti-inflammatory effect by reducing pro inflammatory cytokine expression, blocking leucocyte adhesion and decreasing oxidative stress due to infection. The combination of therapy may reduce the bile acid cytotoxicity of bile and, possibly, decrease of the concentration of hydrophobic bile acids in the cholangiocyte.[20] The whole treatment regimen may be due to increase the conjugation of bile and increase own detoxification. All of the drugs have properties srotosodhaka which may increase the bile flow without increase biliary pressure by cholestasis resolution. Similar outcome are observed in modern literature and one Korean herbal.[10], [21]
Conclusion
This case report is preliminary evidence for further stresses the significance of Siddha Makardwaja Rasayana along with other Ayurveda formulations in early remission of high bilirubin and liver transaminase in Hepatitis A infection. This treatment regimen can be used for local epidemic of Hepatitis A for appropriate Ayurveda management after randomised clinical trial.
Patient Consent
The patient was given his consent to publish his investigation reports and other related information in journal for academic purposes.
Source of Funding
None.
Conflict of Interest
None.
References
- . World Health Organization. Hepatitis A. In: World Health Organization. . . [Google Scholar]
- Alebaji M, Mehair A, Shahrour O, Elkhatib F, Alkaabi E, Alkuwaiti N. Prolonged Cholestasis Following Acute Hepatitis A Infection: Case Report and a Review of Literature.. Cureus. 2023;15(5). [Google Scholar]
- Jayappa M, Kumar P, Goyal J. Prolonged cholestasis after acute viral hepatitis: successfully treated with oral steroid. BMJ Case Rep. 2020;13(5). [Google Scholar]
- Chandrakumar A, Xavier A, Xavier A, Manakkadiyil A, Reghu A, Thomas L. Implications of traditional medicine in the treatment of Hepatitis A in Kerala. J Tradit Complement Med. 2009;6(3):316-36. [Google Scholar]
- Panda A, Sahoo P. Role of Krimi (Pathogen) in AupasarkikaYakrit Vikara (Infective Liver diseases) - A Narrative Review. J Ayurveda Integr Med Sci. 2020;4(2):204-10. [Google Scholar]
- Raval P, Raval R. Treatment of infective hepatitis: Where biomedicine has no answers, Ayurveda has!! Anc Sci Life. Ancient Sci Life. 2016;35(3):176-85. [Google Scholar]
- Park C, Lee G, Son C, Cho J, Lee N. Recovery from hepatitis A after Korean medicine-based treatment: a case report. Integr Med Res. 2019;8(4):257-60. [Google Scholar]
- Foster A, Hernandez S. Hepatitis A: A Case Report Example of a Growing Epidemiological Threat. Spartan Med Res J. 2019;4(3). [Google Scholar]
- Seo D, Lee M, Jeon S, Park H, Jeong S, Lee B. Antiviral activity of herbal extracts against the hepatitis A virus. Food Control. 2017;72(A):9-13. [Google Scholar]
- Lee M, Lee B, Lee S, Choi C. Reduction of hepatitis a virus on frhk-4 cells treated with Korean red ginseng extract and ginsenosides. J Food Sci. 2013;78(9):1412-5. [Google Scholar]
- Panda A, Das D, Dixit A. Hazra J Rapid clearance of HbsAg and liver transaminase in hepatitis B infection with classical Ayurvedic formulation: case study. Asian J Phytomed Clin Res. 2015;3(1):1-5. [Google Scholar]
- Stickel F, Schuppan D. Herbal medicine in the treatment of liver diseases.. Dig Liver Dis. 2007;39(4):293-304. [Google Scholar]
- Panda K, Kar S, Makardwaja S. Phyllanthus niruri) can reverse the progression of Non Alcoholic Steato-hepatitis(NASH): Case study. J Pre Med Hol Health. 2024;10(1):37-40. [Google Scholar]
- Antarkar D, Vaidya A, Doshi J, Athavale A, Vinchoo K, Natekar M. A double-blind clinical trial of Arogyawardhani- an ayurvedic drug-in acute viral hepatitis. Indian J Med Res. 1980;72:588-93. [Google Scholar]
- Jha V, Kumar A, Yadav R. Comparative study to evaluate clinical profile and outcome in Hepatitis-B patients receiving tenofovir therapy compared to traditional herbal therapy( LiV 52HB). Medplus Int J Med. 2021;19(3):106-11. [Google Scholar]
- Panda A, Tripathy R. Inflammation): critical review. Int J Res Granthalaya. 2020;8(8):15-23. [Google Scholar]
- Kumar N, Singh A. Phalatrikadi Kasaya- An Ayurvedic hepato protective drug. Int J Res Pharm Chem. 2013;3(3):591-4. [Google Scholar]
- Panda A, Kar S. Siddha Makardwaja and bhumiamalaki (Phyllanthus niruri) can reverse the progression of NonAlcoholic Steato-hepatitis(NASH): Case study. J Prev Med Holistic Health. 2024;10(1):37-40. [Google Scholar]
- Shin E, Jeong S. Natural History, Clinical Manifestations, and Pathogenesis of Hepatitis A. Cold Spring Harb Perspect Med. Cold Spring Harb Perspect Med. 2018;8(9). [Google Scholar]
- Fujita T, Zysman M, Elgrabli D. Anti-inflammatory effect of gold nanoparticles supported on metal oxides. Sci Rep. 2021;11(1). [Google Scholar]
- Shen Y. Chinese fresh herbal medicine in prevention of virus hepatitis A. World J Gastroenterol. 1998;4(2). [Google Scholar]